Presumed Bilateral Ocular Tuberculosis in a Young Patient - Diagnostic Approach and Follow-Up: Case Report
Article Sidebar
Main Article Content
Abstract
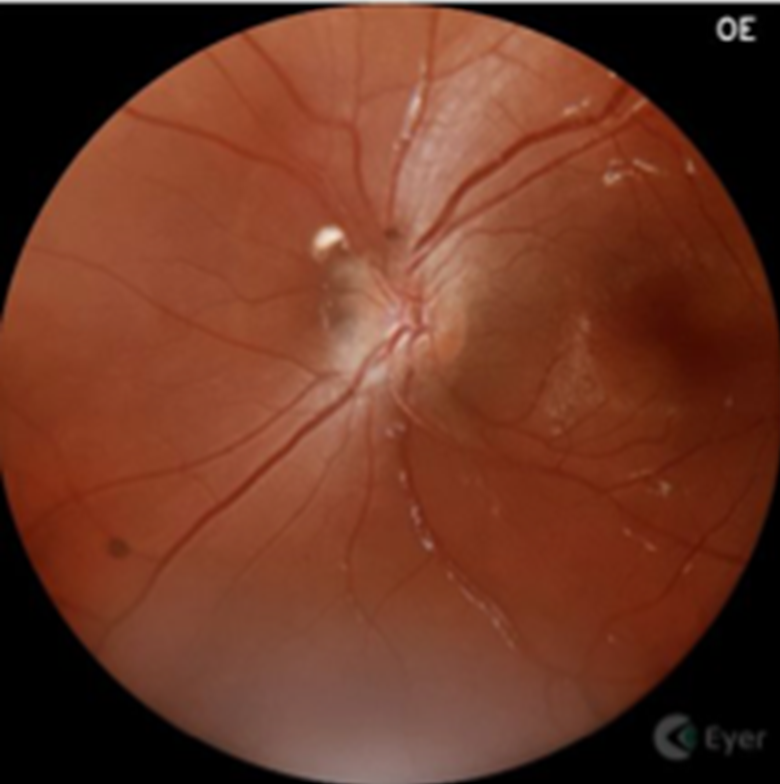
Ocular tuberculosis is a rare extrapulmonary manifestation of Mycobacterium tuberculosis infection, which may occur even in the absence of other apparent foci of the disease. Early diagnosis is crucial to prevent irreversible visual complications, especially in young patients. To report a case of presumed bilateral ocular tuberculosis in a young patient without prior history of tuberculosis or other evident foci, highlighting clinical, laboratory, therapeutic, and follow-up aspects. A qualitative and descriptive case report based on retrospective analysis of medical records, ophthalmic imaging, and laboratory results. The patient underwent fundus photography, optical coherence tomography (OCT), and laboratory testing including serologies for toxoplasmosis, syphilis, and IGRA. The patient presented with bilateral granulomatous chorioretinal lesions morphologically consistent with choroidal tuberculomas. Based on compatible clinical findings, exclusion of other etiologies, and a positive IGRA, a diagnosis of possible intraocular tuberculosis was established. She was started on the WHO-recommended four-drug antituberculosis regimen (isoniazid, rifampicin, pyrazinamide, and ethambutol) without adjuvant corticosteroids. After six months of follow-up, uncorrected visual acuity (UCVA) in the right eye improved from 20/200 to 20/40, with partial regression of the lesion adjacent to the optic disc on OCT. The left eye maintained 20/20 UCVA with stable perimacular findings. This case highlights the importance of considering presumed ocular tuberculosis as a diagnostic possibility even in the absence of pulmonary foci or prior history of the disease. Early diagnosis and appropriate multidisciplinary follow-up were essential for controlling intraocular inflammation and preventing permanent visual sequelae.
Article Details

This work is licensed under a Creative Commons Attribution 4.0 International License.
Authors retain the copyright of their articles and grant the journal the right of first publication under the Creative Commons Attribution (CC BY) license, which allows others to share and adapt the work with proper attribution.
References
Shakarchi FI. Ocular tuberculosis: current perspectives. Clin Ophthalmol. 2015;9:2223–2227. PMID: 26648690
Agarwal A, Majumder PD, Biswas J. Current approach in the diagnosis and management of posterior uveitis. Indian J Op-hthalmol. 2020;68(9):1796–807.
Agrawal R, et al. Diagnostic challenges in tubercular uveitis. Int Ophthalmol Clin. 2015;55(2):1–21. PMID: 25702372.
Bansal R, et al. Current approach in the diagnosis and management of presumed tubercular uveitis. Indian J Ophthalmol. 2015;63(8):556–560. PMID: 26305079.
Bodaghi B, et al. Ocular tuberculosis: clinical presentation and management. Ocul Immunol Inflamm. 2005;13(6):451–461. PMID: 16382870.
Gupta A, et al. Tuberculosis of the eye. Int Ophthalmol Clin. 2005;45(2):65–76. PMID: 15805920.
Ang M, et al. Interferon gamma release assay for the diagnosis of tuberculous uveitis: a meta-analysis. Br J Ophthalmol. 2012;96(2):200–205. PMID: 21712337.
Mazumder SA, et al. Update on the use of interferon-gamma release assays in the diagnosis of tuberculosis infection. Curr Opin Infect Dis. 2010;23(3):246–251. PMID: 20375790.
Vasconcelos-Santos DV, et al. Ocular tuberculosis in immunocompetent patients: a Brazilian perspective. Ocul Immunol In-flamm. 2021;29(4):823–831. PMID: 34482752.
Herbort CP, et al. Differentiating ocular sarcoidosis from tuberculosis in endemic areas: the COTS consensus. Int Ophthalmol. 2022;42:2873–2882. PMID: 36188648.
Bansal R, et al. Role of corticosteroids in management of tubercular uveitis. Ocul Immunol Inflamm. 2015;23(1):1–6. PMID: 25565286.